
A slight curve to the penis is normal. Most men have one to some degree and it causes no problems. Peyronie’s disease is different. It involves the formation of fibrous scar tissue, called plaque, inside the penis that causes a significant bend, pain during erections, and in many cases difficulty with sexual intercourse. The condition affects an estimated 6% to 10% of men, most commonly between the ages of 40 and 70, though it can develop earlier. At Lazare Urology in Brooklyn, Dr. Jon Lazare treats Peyronie’s disease across its full spectrum, from early-stage cases that respond to medication to advanced curvature that requires surgical correction.
Men often wait a long time before seeking help, partly because the condition feels embarrassing and partly because they assume nothing can be done. Both assumptions are wrong.
What Causes Peyronie’s Disease and How It Progresses
The exact cause isn’t fully understood, but the prevailing theory is that Peyronie’s begins with trauma to the penis, often minor and unnoticed, during sexual activity or physical impact. In most men, this kind of micro-injury heals normally. In men who develop Peyronie’s, the healing process produces excess scar tissue that forms a hard, flat plaque beneath the skin of the penis. Genetics likely play a role in determining who is susceptible. Men with Dupuytren’s contracture (a thickening of tissue in the palm of the hand) are at higher risk, suggesting a shared predisposition to abnormal scarring.
The disease typically progresses through two phases.
The acute phase lasts roughly 6 to 18 months. During this period, the plaque is still forming, the curvature may be changing, and erections are often painful. The pain is caused by inflammation around the developing scar tissue. For most men, this is when the condition first becomes noticeable, either because of pain, a new bend they hadn’t seen before, or both.
The stable phase begins once the plaque has matured and the curvature stops progressing. The pain usually resolves by this point, but the bend remains. For some men the curvature is mild enough that it doesn’t interfere with sexual function. For others, the degree of bending, shortening, narrowing, or indentation makes intercourse physically difficult or impossible. Erectile dysfunction frequently accompanies Peyronie’s, either because the plaque itself restricts blood flow or because the psychological impact of the condition undermines confidence and arousal.
Peyronie’s does not resolve on its own in the majority of cases. Studies tracking natural progression show that about 12% of men experience spontaneous improvement, roughly 40% remain stable, and the rest worsen over time.
Non-Surgical Treatment: Xiaflex
Xiaflex (collagenase clostridium histolyticum) is the only FDA-approved medication for Peyronie’s disease. It’s an injectable enzyme that breaks down the collagen in the plaque, softening the scar tissue and allowing the curvature to improve over a series of treatments.
The standard Xiaflex protocol involves up to four treatment cycles, each consisting of two injections spaced one to three days apart followed by a penile modeling exercise performed in the office and at home. Modeling involves gently bending the penis in the opposite direction of the curvature to stretch and remodel the treated plaque. A full course of treatment spans several months.
Xiaflex is most effective for men with a palpable plaque and a curvature between 30 and 90 degrees who are in the stable phase of the disease. It won’t completely eliminate the curvature in most cases, but clinical trials showed an average improvement of about 34% in penile curvature, which for many men is enough to restore functional intercourse.
The treatment is not appropriate for plaques that involve calcification (hardened, calcium-laden scar tissue) or for curvature caused by a ventral plaque (on the underside of the penis near the urethra), due to the risk of injury to the urethra during injection. Dr. Lazare evaluates plaque location and composition through physical examination and sometimes ultrasound before recommending Xiaflex.
Side effects are generally localized: bruising, swelling, and soreness at the injection site are common and resolve within a couple of weeks. The most serious risk is penile fracture or rupture of the corpus cavernosum, which is rare but requires immediate surgical repair. Patients are advised to avoid sexual activity for two weeks after each injection cycle.
Surgical Options for Advanced Peyronie’s Disease
When the curvature is too severe for Xiaflex, when the plaque is calcified, or when the patient has already tried injection therapy without adequate improvement, surgery becomes the recommended path. Dr. Lazare offers two primary surgical approaches at Lazare Urology, and the choice between them depends on the degree of curvature, penile length, and erectile function.
Penile Plication
Plication is the simpler of the two surgeries. It involves placing permanent sutures on the side of the penis opposite the plaque, effectively shortening the longer side to match the shorter, curved side. Think of it as straightening a bent piece of metal by compressing the convex side rather than stretching the concave side.
The advantage of plication is that it’s technically straightforward, has a low complication rate, and doesn’t involve grafting or cutting into the plaque itself. The trade-off is some degree of penile shortening, because you’re bringing the longer side down to match the shorter side. For men with moderate curvature (typically under 60 degrees) and adequate penile length, the shortening is usually acceptable and the results are reliable.
Plication is performed under sedation in Dr. Lazare’s in-office operating room and typically takes about an hour. Recovery involves several weeks of restricted activity, with sexual intercourse off limits for approximately six weeks.
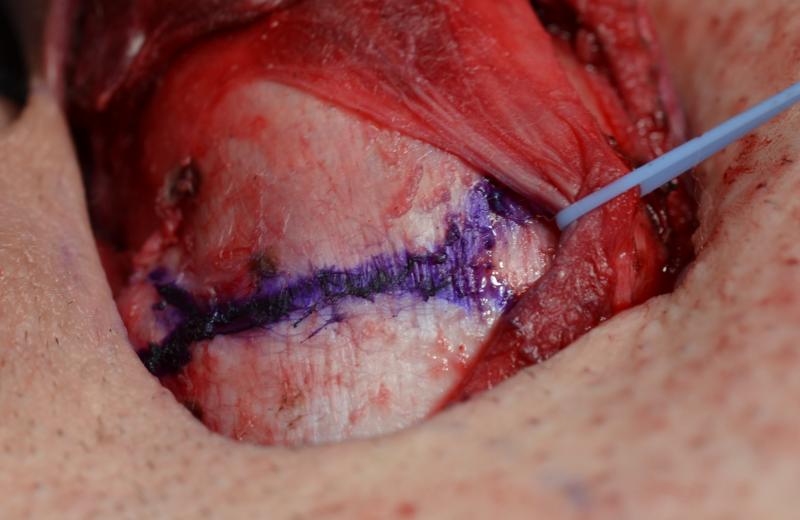
Plaque Excision with Grafting
For men with severe curvature (generally above 60 degrees), significant penile shortening from the disease itself, or complex deformities like hourglass narrowing or hinge defects, plaque excision with grafting is the more appropriate option. The surgeon makes an incision into the plaque, partially or fully removes the scar tissue, and patches the resulting defect with a graft material. The graft allows the shorter side of the penis to be lengthened, correcting the curvature while preserving or restoring penile length.
This is a more complex surgery that takes longer and has a more involved recovery. The grafting material can come from several sources, including processed human or animal tissue grafts. Dr. Lazare discusses the specific graft options during the consultation and recommends the material best suited to the defect being repaired.
Plaque excision with grafting carries a higher risk of post-operative changes in sensation and, in some cases, erectile dysfunction compared to plication. For this reason, it’s generally reserved for men who have good pre-operative erectile function, since the procedure’s benefit depends on the ability to achieve erections afterward. Men with Peyronie’s disease who also have significant erectile dysfunction may be better served by a penile implant, which straightens the penis and restores rigidity simultaneously.
How Lazare Urology Approaches Peyronie’s Treatment
Peyronie’s disease requires a tailored approach because no two cases present identically. The degree of curvature, the location and composition of the plaque, the presence or absence of erectile dysfunction, and the patient’s priorities around length preservation all factor into the treatment plan. Dr. Lazare evaluates each of these variables during the consultation and recommends the option that gives the best balance of correction, function, and realistic expectations.
If you’re dealing with penile curvature that’s affecting your confidence or your ability to have sex, waiting rarely makes things better. Contact Lazare Urology at (718) 568-7516 to schedule a consultation. Dr. Lazare will assess your condition, explain which treatment options apply to your specific case, and answer the questions you’ve been hesitant to ask.

